

Can Patients Participate In Cardiac Rehab If Receiving Home Health Services
Original Editor Rachael Lowe
Top Contributors - Magdalena Hytros, Garima Gedamkar, Adam Vallely Farrell, Admin, Kim Jackson, Vidya Acharya, Rachael Lowe, Lucinda hampton, WikiSysop, Simisola Ajeyalemi, Evan Thomas, Naomi O'Reilly, Tarina van der Stockt and Karen Wilson
Introduction [edit | edit source]

Cardiovascular disease (CVD) is one of the leading causes of death worldwide and is the leading cause of death in the United States.
Cardiac rehabilitation is a complex, interprofessional intervention customized to individual patients with various cardiovascular diseases such as:
- Coronary artery disease (CAD),
- Heart failure
- Myocardial infarctions
- Patients who have undergone cardiovascular interventions such as coronary angioplasty or coronary artery bypass grafting[1].
Cardiac rehabilitation program [edit | edit source]
Cardiac rehabilitation programs aim to limit the psychological and physiological stresses of CVD, reduce the risk of mortality secondary to CVD, and improve cardiovascular function to help patients achieve their highest quality of life possible. Accomplishing these goals is the result of improving overall cardiac function and capacity, halting or reversing the progression of atherosclerotic disease, and increasing the patient's self-confidence through gradual conditioning[1]
CR ere the process by which patients with cardiac disease, in partnership with a multidisciplinary team of health professionals are encouraged to support and achieve and maintain optimal physical and psychosocial health. The involvement of partners, other family members, and carers is also important"[2]
They require a team approach, including a multidisciplinary the multidisciplinary team including:
-
- Cardiologist/Physician and co-coordinator to lead cardiac rehabilitation
- Clinical Nurse Specialist
- Physiotherapist
- Clinical nutritionist/Dietitian
- Occupational Therapist
- Pharmacist
- Psychologist
- Smoking cessation counselor/nurse
- Social worker
- Vocational counselor
- Clerical Administration[3]
It is essential that all cardiac rehabilitation staff have appropriate training, qualifications, skills, and competencies to practice within their scope of practice and recognise and respect the professional skills of all other disciplines involved in providing comprehensive cardiac rehabilitation. The cardiac rehabilitation team should actively engage and effectively link with the general practitioner and practice nurses, sports and leisure industry where phase IV is conducted, community pharmacists and other relevant bodies to create a long-term approach to CVD management.[4]
Description [edit | edit source]
[5]
Indication [edit | edit source]
Cardiac rehabilitation should be offered to all cardiac patients who would benefit:[6]
- Recent myocardial infarction
- Acute coronary artery syndrome
- Chronic stable angina
- Congestive heart failure
- After coronary artery bypass surgery
- After a percutaneous coronary intervention
- Valvular surgery[1]
- Cardiac transplantation
CR begins as soon as possible in intensive care units (only if the patient is in stable medical condition). Intensity of rehabilitation depends on the patient's condition and complications in the acute phase of disease.[7] Randomized controlled trials and systematic analysis show that early mobilization improved physical function (distance walked during the 6-min walking test improved by 54 m) at the discharge in patients after cardiac surgery.[8] Another prospective randomized clinical trial improved postoperative functional capacity (6-minute walk test) shorten the duration of mechanical ventilation, dependence on oxygen therapy, and reduced the time of hospital stay in patients who underwent elective Coronary artery bypass graft surgery[9].
Goals of Cardiac Rehabilitation [edit | edit source]
Comprehensive cardiac rehabilitation program should contain specific core components.
These components should optimize cardiovascular risk reduction, reduce disability, encourage active and healthy lifestyle changes, and help maintain those healthy habits after rehabilitation is complete. Cardiac rehabilitation programs should focus on:
- Patient assessment nutritional counseling
- Weight management
- Blood pressure management
- Lipid management
- Diabetes management
- Tobacco cessation
- Psychosocial management
- Physical activity counseling
- Exercise training[1]
Individual Risk Assessment [edit | edit source]
CR can be tailored to meet individual needs thus a thorough assessment and evaluation of the CV risk factor profile of the patient should be undertaken at the beginning of the programme. This should be accompanied by ongoing assessment and reassessment throughout and upon completion of the programme.[4]
Risk factors should be evaluated using validated measures which take into account other co-morbidities[2] [3] [10].
| RISK FACTORS | |
|---|---|
| Non Modifiable | Modifiable |
| Age | Excessive alcohol intake |
| Gender | Dyslipedemia |
| Personal Cardiac History | Hypertension |
| Family History of CVD | Obesity |
| Diabetes (unless prediabetes) | Smoking |
| Physical Inactivity | |
| Anxiety/Depression | |
| Hostility | |
| Stress | |
Other factors to consider
- Family Support
- Social History
- Occupation
Cardiac Rehabilitation Participation [edit | edit source]
Participation in cardiac rehabilitation programs should be available to all cardiac patients who require it. Age is not and should not be a barrier to cardiac rehabilitation participation[4]. However, consideration of patient safety results in the following specific inclusion/exclusion criteria applying to participation in the Phase III exercise component.[11]
| Inclusion | Exclusion |
| Medically stable post MI | Unstable Angina |
| Coronary Artery Bypass Surgery | Ischaemic changes on ECG |
| Percutaneous Coronary Intervention | Resting systolic BP >200mmHg or resting diastolic BP >110 mmHg |
| Stable Angina | Orthostatic BP drop >10mmHg with symptoms |
| Stable heart failure (NYHA I-III) | Critical aortic stenosis (peak pressure gradient >50mmHg with aortic valve orifice <0.75cm2 |
| Cardiomyopathy | Acute systemic illness or fever |
| Cardiac Transplantation | Uncontrolled atrial or ventricular arrhythmias |
| Implantable Cardioverter Defibrillator | Uncontrolled sinus tachycardia (>120bpm) |
| Valve Repair/Replacement | Uncompensated CHF |
| Insertion of Cardiac Pacemaker (with one or more other inclusion criteria) | Acute systemic illness |
| Peripheral Arterial Disease | 3rd degree AV block with no pacemaker |
| Post Cerebral Vascular Disease | Acute pericarditis/myocarditis |
| At risk of coronary artery disease with diagnosis of diabetes, dyslipedemia, hypertension | Recent embolism |
| Thromobophlebitis | |
| Uncontrolled diabetes | |
| Severe orthopediac problems | |
| Other metabolic problems such as acute thyroiditis, hypo-hyperkalaemia, hypovolemia |
Phases of Cardiac Rehabilitation [edit | edit source]
Cardiac rehabilitation consists of 3 phases.
Phase I: Clinical phase
This phase begins in the inpatient setting soon after a cardiovascular event or completion of an intervention. It begins by assessing the patient's physical ability and motivation to tolerate rehabilitation. Therapists and nurses may start by guiding patients through non-strenuous exercises in the bed or at the bedside, focusing on a range of motion and limiting hospital deconditioning. The rehabilitation team may also focus on activities of daily living (ADLs) and educate the patient on avoiding excessive stress. Patients are encouraged to remain relatively rested until completion of treatment of comorbid conditions, or post-operative complications. The rehabilitation team assesses patient needs such as assistive devices, patient and family education, as well as discharge planning.
Phase II: Outpatient cardiac rehab
Once a patient is stable and cleared by cardiology, outpatient cardiac rehabilitation may begin. Phase II typically lasts three to six weeks though some may last up to up to twelve weeks. Initially, patients have an assessment with a focus on identifying limitations in physical function, restrictions of participation secondary to comorbidities, and limitations to activities. A more rigorous patient-centered therapy plan is designed, comprising three modalities: information/advice, tailored training program, and a relaxation program. The treatment phase intends to promote independence and lifestyle changes to prepare patients to return to their lives at home.
Phase III: Post-cardiac rehab. Maintenance
This phase involves more independence and self-monitoring. Phase III centers on increasing flexibility, strengthening, and aerobic conditioning.
Goal: facilitate long term maintenance of lifestyle changes, monitoring risk factor changes and secondary prevention.[12]
Options:
- Educational sessions
- Support groups
- Telephone follow up
- Review in clinics
- Outreach programmes
- Exercise program organised by qualified phase IV gym instructor
- Links with GP and primary health care team
- Ongoing involvement of partners/spouses/family[4]
A randomized controlled study shows positive outcomes with the internet-based remote home-based cardiac rehabilitation program[13]
NB There is also a pre-surgery phase, where the patient starts cardiovascular rehabilitation. A small number of studies demonstrate that the post-surgical pathway is better tolerated by patients[1].
Sample format of a cardiac rehabilitation class [edit | edit source]
- Check in (vitals assessed)
- Warm Up (15 mins)
- Main class (30 mins)
- Cool down (10 mins)
- Monitoring and reassessment of vitals and check out
[14]
Warm-Up [edit | edit source]
Purpose: Prepare the body for exercise by raising the pulse rate in a graduated and safe way
Effects:
- redistributes blood to active tissues
- increases muscle temperature and speed of muscle action and relaxation
- prepares the mind
- prepares the muscle for the ROM involved for the conditioning period
Should include pulse raising activities (5 minutes) eg) marching on the spot, walking, low-level cycle followed by stretching of the major muscle groups (5 mins) followed by more pulse raising activity.
NB: should try to keep feet moving at all times to maintain HR and body temp and avoid pooling.
Main Class [edit | edit source]
For group rehab circuit training seems most popular. Depending on CV status and functional capacity patients may adopt an interval or continuous approach to the circuit.
Separate stations are set out and participants spend a fixed amount of time at each aerobic station (30secs-2mins) before moving onto the next station which may be rest or active recovery in the form of resistance work targeted at specific muscle groups.
Resistance work as set out by ACSM 2006 – 10-15 reps to moderate fatigue of 8-10 exercises.[15] [16]
Individualisation of the CV component can be achieved by varying; duration spent at each CV station, intensity (increase resistance, speed or ROM), period of rest, overall duration of the class[17]
Cool Down [edit | edit source]
10 minutes at the end
Goal: bring the body back to its resting state
Should incorporate movements of diminishing intensity and passive stretching of the major muscle groups.
Necessary because of;
- Increased risk of hypotension
- Older hearts take longer to return to resting levels
- Raised sympathetic activity during exercise increases the risk of arrhythmias immediately post exercise.[17]
Health and Safety [edit | edit source]
A study in France reviewing the safety of cardiac rehabilitation found the cardiac arrest rate was 1.3 per million patient hours of exercise[1]
Patient shouldn't exercise if they are generally unwell, symptomatic or clinically unstable on arrival;
- Fever/acute systemic illness
- Unresolved/unstable angina
- Resting BP systolic >200mmHg and diastolic > 110mmHg
- Significant drop in BP
- Symptomatic hypotension
- Resting/uncontrolled tachycardia (>100bpm)
- Uncontrolled atrial or ventricular arrhythmias
- New/recurrent symptoms of breathlessness, lethargy, palpitations, dizziness
- Unstable heart failure
- Unstable/uncontrolled diabetes[18] [4]
Need to consider the following;
- Local written policy clearly displayed for the management of emergency situations
- Rapid access to emergency team in hospital or via ambulance
- Regular checking and maintenance of all equipment
- Drinking water and glucose supplements available as required
- Access to and from venue, emergency exits, toilets and changing areas, lighting, surface and room space checked to ensure they're appropriate
- Enough space for patient traffic and safe placement of equipment
- Adequate temperature and ventilation
- Medications of patients and their associated effects
Assessment and Outcome Measures [edit | edit source]
It is essential to;
- set and evaluate the effectiveness of an exercise programme
- provide objective feedback to the patient
- facilitate evidence-based practice
Measures can be used as both a baseline measure and exit outcome measure. These may include;
- HR and BP @ rest and during exercise
- RPE
- Bodyweight
- BMI
- Waist circumference
Measures of functional capacity;
- 6MWT
- shuttle walk test
- chester step test
Exercise Testing and Risk Stratification [edit | edit source]
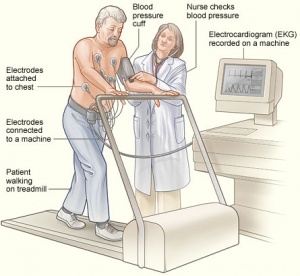
A patient having a stress test. Electrodes are attached to the patient's chest and connected to an EKG machine. The EKG records the heart's electrical activity. A blood pressure cuff is used to record the patient's blood pressure while he walks on a treadmill.[19]
EACPR, ACCPVR, CACR, ESC and AHA all recommend exercise testing as part of a patient's initial assessment for cardiac rehabilitation. Exercise testing allows for the following;
- Diagnosis – identification of patients with CHD and the severity of the disease
- Prognosis – identification of low, moderate and high risk patients
- Evaluation – establishment of the effectiveness of a selected intervention
- Measurement of functional capacity – used as a basis for advice re ADLs and development of a formal exercise prescription
- Measurement of acute exercise responses – BP, HR, ventilator responses and detection of exercise induced arrhythmias
- To provide an appropriate training target HR[16]
Exercise ECG using an incremental protocol is most commonly used and before acceptance into the phase III programme a symptom limited test is customary. Usually uses the Bruce Protocol
Criteria for terminating a test[16]:
| Horizontal or downsloping ST segment depression >2mm – indicates ischaemia |
| Marked drop in systolic BP >20mmHG – indicates poor LV fxn or severe coronary disease |
| Serious arrhythmias – ventricular tachycardia |
| Patient fatigue and/or excessive breathlessness at low workloads – poor fxnl capacity or more serious problems such as heart failure |
| Negative Test | Positive Test |
| Normal haemodynamic response | Significant ECG changes |
| Completion of a workload equivalent to the second stage of the Bruce protocol (7 METs) | Inappropriate HR/BP response to the incremental workload. |
NB: when carrying out the test patients HR, BP and 12 lead ECG must be constantly assessed. Once test has terminated recovery monitoring must be continues for a minimum of 6 secs or until the ECG returns to its pretest appearance.[16]
Risk Stratification [11] [edit | edit source]
Definition: "Evaluation of the patient to assess the degree of risk of future cardiac events associated with exercise" [2]
| Low Risk (all characteristics listed must be present to remain @ lowest risk) | Moderate Risk (any one or a combination of these findings) | High Risk (anyone or a combo) |
| Uncomplicated MI, CABG, angioplasty | Functional capacity <5-6 METs | Severely depressed LV function |
| Funct. Capacity >6 METs | Mild – moderate depressed LV dysfunction (EF 31-49%) | Complex arrhythmias @rest or during exercise) |
| No resting/exercise induced complex arrhythmias | Mild – moderate ischaemia in exercise/recovery | Decreased systolic BP of >15mmHg during exercise/ failure of BP to rise consistently with exercise workloads |
| No sig. LV dysfunction (EF >50%) | Exercise induced STsegment depression of 1-2mm or reversible ischaemic effects | MI complicated by CHF/cardiogenic shock/complex ventricular arrhythmias |
| Normal heamodynamic response during exercise | Presence of angina or relevant symptoms at high levels of exertion (>7 METs) | Severe CAD and marked (>2mm) exercise induced ST segment depression |
| Absence of CHF | Survivor of cardiac arrest | |
| Absence of angina/other sig symptoms | Complicated MI or revascularisation procedure | |
| Absence of clinical depression | Presence of clinical depression |
Risk stratification is important as it will have a bearing on staffing required and group mixing. It's also something that has to be taken into account when determining the level of monitoring a patient requires and when setting their Target Training HR.
Requirements for cardiac rehabilitation [edit | edit source]
Facilities and Equipment [edit | edit source]
The minimum facilities necessary to provide a cardiac rehabilitation service are:
- Separate office space and facilities for cardiac rehabilitation staff
- An Education Room furnished with seats, TV and DVD player and with a selection of information booklets and DVD's provided. The size of the education room will depend upon the number of participants (patients, spouses, and staff) in the education sessions and given resources.
- It is recommended that the exercise warm-up area and the exercise room combined should be approximately 300m2
- The exercise room should be air-conditioned
- In addition, patients should have access to
- Toilet
- Shower and changing room
- Available drinking water[4]
Equipment in the exercise room may include[4]
| Central monitor and telemetry | Treadmill | Versa climber | Chairs | Music system |
| Equipped emergency trolley, portable suction, defibrillator and oxygen | Dual cycle ergometer | Hand crank | Rowing Machine | Glucometer |
| Automated Blood Pressure Recording Machine e.g. Dinamap | Bicycle ergometer | Multigym weights system and/or dumb bells | Stethoscope | Measuring tape |
Staffing Levels [edit | edit source]
ACPICR 2009 – minimum staff to patient ratio should be 1:5 but this will vary depending on the risk stratification profile of the class. For higher risk patients will have increased staff ratio eg) 1:3
SIGN 2002 guidelines: Staff should have basic life support training and the ability to use a defribillator required for low-moderate risk patients[2]
Future Research [edit | edit source]
Finding in a systematic review of 19 random clinical trials on complex e-coaching
- Found e-coaching to be an effective method of delivering therapies targeting physical capacity, clinical status, and psychosocial health (detailed protocols were not well described).
- Determining which aspects of e-coaching have the most benefit need to be further developed.
- Basic e-coaching was not found to be effective. [1]
According to the analysis (April 2020) of Indian data from the global cardiac rehabilitation (CR) audit and survey, conducted by the International Council of Cardiovascular Prevention and Rehabilitation (ICCPR), the need for CR is highest in India. Research indicates a lack of patient referral and financial resources as barriers to programs. Healthcare provider training and financially supported by the government can make CR delivery in India better[20].
Resources [edit | edit source]
- BACPR
- SIGN Guidelines
- Cardiac Rehabilitation: Putting More Patients on the Road to Recovery, American Heart Association, May 2017.
- Cardiac Rehabilitation podcast, BMJ Talk Medicine, 2015
References [edit | edit source]
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 1.6 Tessler J, Bordoni B. Cardiac Rehabilitation. InStatPearls [Internet] 2019 Sep 9. StatPearls Publishing.Available from:https://www.ncbi.nlm.nih.gov/books/NBK537196/ (last accessed 9.8.2020)
- ↑ 2.0 2.1 2.2 2.3 Scottish Intercollegiate Guidelines Network (SIGN) Cardiac rehabilitation: a national clinical guideline, 2002
- ↑ 3.0 3.1 American Association of Cardiovascular and Pulmonary Rehabilitation Robertson, L (Ed.) (2006) Cardiac Rehabilitation Resource Manual. Champaign: Human Kinetics.
- ↑ 4.0 4.1 4.2 4.3 4.4 4.5 4.6 Irish Association of Cardiac Rehabilitation Guidelines 2013
- ↑ SSM Health St. Mary's Hospital – Madison Cardiac Rehab Program Available from: https://www.youtube.com/watch?v=famkb_dtAF0&feature=emb_logo
- ↑ Pryor JA, Prasad SA. Physiotherapy for Respiratory and Cardiac Problems. Philadelphia: Elsevier Ltd, 4th Edition, 2008: 14 (470 - 494).
- ↑ Cardiac rehabilitation. Available from: http://www.pnmedycznych.pl/spnm.php?ktory=369 (accessed 22.12.2013)
- ↑ Kanejima Y, Shimogai T, Kitamura M, Ishihara K, Izawa KP. Effect of Early Mobilization on Physical Function in Patients after Cardiac Surgery: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2020 Jan;17(19):7091.
- ↑ Sahar W, Ajaz N, Haider Z, Jalal A. Effectiveness of Pre-operative Respiratory Muscle Training versus Conventional Treatment for Improving Post operative Pulmonary Health after Coronary Artery Bypass Grafting. Pakistan Journal of Medical Sciences. 2020 Sep;36(6):1216.
- ↑ British Association of Cardiac Rehabilitation. "Risk Factors" in Brodie, D. ed. (2006) Cardiac Rehabilitation: An Educational resource. Buckinghamshire: Colourways Ltd.
- ↑ 11.0 11.1 American Association of Cardiovascular and Pulmonary Rehabilitation: Guidelines for Cardiac Rehabilitation and secondary prevention programs 2004
- ↑ British Association for Cardiovascular Prevention and Rehabilitation. (2012) The BACPR standards and core components for cardiovascular disease prevention and rehabilitation 2012. 2nd Edition. London: British Cardiovascular Society.
- ↑ Claes J, Cornelissen V, McDermott C, Moyna N, Pattyn N, Cornelis N, Gallagher A, McCormack C, Newton H, Gillain A, Budts W. Feasibility, Acceptability, and Clinical Effectiveness of a Technology-Enabled Cardiac Rehabilitation Platform (Physical Activity Toward Health-I): Randomized Controlled Trial. Journal of Medical Internet Research. 2020;22(2):e14221.
- ↑ British Heart FoundationBritish Heart Foundation - Joining a Cardiac Rehabiltation Programme Available from https://www.youtube.com/watch?v=TRvYqn-a-gk&feature=emb_logo
- ↑ Bjarnason-Wehrens, B. Mayer-Berger, W. Meister, E.R. Baum, K. Hambrecht, R. And Gilen, S. (2004) 'Recommendations for resistance exercise in cardiac rehabilitation. Recommendations of the German Federation for Cardiovascular Prevention and Rehabilitation'. European Journal of Cardiovascular Prevention and Rehabilitation, 11(4):352-61.
- ↑ 16.0 16.1 16.2 16.3 American College of Sports Medicine (2006) Guidelines for Exercise Testing and Prescription. 7th Edition. Baltimore, Maryland: Lippincott Williams & Wilkins.
- ↑ 17.0 17.1 Association of Chartered Physiotherapists in Cardiac rehabilitation (2009) Standards for Physical Activity & Exercise in the Cardiac Population.
- ↑ American Diabetes Association (2013) 'Standards of Medical Care in Diabetes—2013', Diabetes Care, 36: S11-S66.
- ↑ https://www.nhlbi.nih.gov/health/health-topics/topics/stress/during
- ↑ Babu AS, Turk-Adawi K, Supervia M, Jimenez FL, Contractor A, Grace SL. Cardiac Rehabilitation in India: Results from the International Council of Cardiovascular Prevention and Rehabilitation's Global Audit of Cardiac Rehabilitation. Global Heart. 2020;15(1).
Can Patients Participate In Cardiac Rehab If Receiving Home Health Services
Source: https://www.physio-pedia.com/Cardiac_Rehabilitation
Posted by: guoarron1960.blogspot.com
0 Response to "Can Patients Participate In Cardiac Rehab If Receiving Home Health Services"
Post a Comment